
 The play lasted only eight seconds out of 3,600 in the entire game. The distance traveled roughly 16 inches out of 3,600 across the field. Yet what occurred during those 8 seconds and 16 inches could make the difference between immeasurable joy or profound sadness. It all depends on how the referees view the play.
The play lasted only eight seconds out of 3,600 in the entire game. The distance traveled roughly 16 inches out of 3,600 across the field. Yet what occurred during those 8 seconds and 16 inches could make the difference between immeasurable joy or profound sadness. It all depends on how the referees view the play.
Of less substantial consequence in the minds of most Americans, starting tomorrow the Supreme Court will begin hearing arguments over 6 words of the Affordable Care Act – out of roughly 382,000: “through an exchange established by the State.” In November of last year when the Court determined (or at least four Justices did) to hear King v. Burwell I wrote, Does Legislative Negligence Trump Legislative Intent? I discuss there the background and ramifications of this case.
Here I am more interested in briefly sharing some thoughts on the relative influence of sociopolitical factors in SCOTUS’s review and consideration of this case. Whereas our historical view of the Court is one of great reverence and respect – the last bastion wherein ethics and morality trump politics – I think the image I chose for this post today more accurately reflects public opinion of that institution today – right or wrong.
I am not about to argue that politics has only recently become an unsightly element of the Court. Justices are appointed and approved by those who are elected, and they don’t get to the position of being considered by living out an apolitical professional career. From accusations against President Grant for court packing to FDR’s proposal to add members (conjectured to dilute a conservative bench) to more recent skirmishes over presidential nominees (e.g., Bork and Thomas) the Court has been steeped in political undertones for decades.
But what we are witnessing today is beyond just the politicization of appointees and the legacy influences of political ideologies. Like all things touched by our modern media the Court is engulfed by a sea of opinions and editorials in anticipation of a “wrong” decision – having not even heard one word of oral argument. How can the justices not hear the deafening crowd noise any less than the referees on the field looking under the video replay monitor. What influence, if any, will that carry on how they view King v. Burwell?
Regardless of how you hope the case is adjudicated you must see the irony in 8 million lives potentially being negatively impacted by 9 individuals out of 320 million based on the arbitrary interpretation of 6 words among 382,000. Welcome to 21st century democracy in America.
Cheers,
~ Sparky






 Back in the day, before Al Gore had even understood the full impact of his new invention, the Internet was raw and without form. It took the efforts of early technology pioneers who could envision the scalability and acceleration of historic processes. Eric Thomas was an engineering student in Paris back in 1986 when he invented a software program that automated the management of email lists: LISTSERV.
Back in the day, before Al Gore had even understood the full impact of his new invention, the Internet was raw and without form. It took the efforts of early technology pioneers who could envision the scalability and acceleration of historic processes. Eric Thomas was an engineering student in Paris back in 1986 when he invented a software program that automated the management of email lists: LISTSERV.

 Over the period January 8th through the 11th of last week the Morning Consult
Over the period January 8th through the 11th of last week the Morning Consult 
 In the poem, Ode on a Distant Prospect of Eton College, Thomas Gray wrote that, "where ignorance is bliss, ’tis folly to be wise." He was referring to the unfettered ability of time to ultimately win any race against human pain and sorrow – and since that race is determined before it is run, why not walk and enjoy what you may. Or something like that.
In the poem, Ode on a Distant Prospect of Eton College, Thomas Gray wrote that, "where ignorance is bliss, ’tis folly to be wise." He was referring to the unfettered ability of time to ultimately win any race against human pain and sorrow – and since that race is determined before it is run, why not walk and enjoy what you may. Or something like that.



{kind=link}
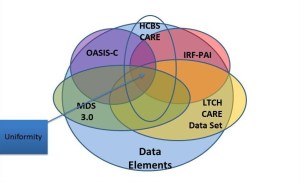
The core challenge is in the one size fits all model of healthcare that currently exists. The system as a…
Reblogged this on rennydiokno.com.
I think you're absolutely right, Scot. We've passed the point of no return on Federal dysfunction.
It sounds like violence can change one's mind about what is right and what is wrong. I always thought that…
The important issue is not the comment that Gruber made rather the fact that he and the administration intended to…