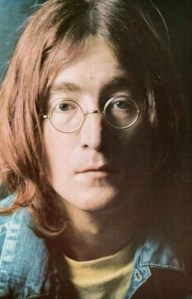

On December 9th, 1980 this image was hastily taped to a window in a basement dorm room of Pacelli Hall at John Carroll University. It was a Tuesday. I was living in the basement of Pacelli Hall. Or supposed to be, anyway.
The evening before I spent upstairs at my parents’ house where I had been studying (or what then I thought was studying) and listening to WMMS. DJ Denny Sanders interrupted a song to share that John Lennon had been shot. It didn’t sink in. It couldn’t.
A bit later another broadcast interruption shared that John Lennon had died. DIED? As in, he’s not going to be here tomorrow? Who would want to kill John Lennon? What did he ever do to someone to deserve that?
I will never (hopefully) forget the image of that dismal day in Cleveland. It was the kind of day that you have to live here long enough to despondently appreciate the experience. Dark. Rain. Fog. Just cold enough to where rain doesn’t turn to snow.
God had brought forth the perfect ambiance for mourning. John Lennon had died. And with him another slice of our youthful innocence. December 8th is rightly remembered as a tragic day in our country’s lexicon. December 9th was the day we had to begin reconciling a shared tragedy with our own will to live.

 The James Comey Oval Office conversation looks like a
The James Comey Oval Office conversation looks like a 

 If you are a post-acute/long-term care provider still sitting on the sidelines waiting for a clearer understanding of how Healthcare Reform is going to impact your organization’s future, well then all I can say is, “Good luck with that – let me know how it works out for you.”
If you are a post-acute/long-term care provider still sitting on the sidelines waiting for a clearer understanding of how Healthcare Reform is going to impact your organization’s future, well then all I can say is, “Good luck with that – let me know how it works out for you.”

 I started Sparky’s Policy Pub back in May because I believed it would be a productive and enjoyable means of sharing information, thoughts, opinions and insights on public policy issues likely to impact providers of affordable housing, aging services and post-acute/long-term care.
I started Sparky’s Policy Pub back in May because I believed it would be a productive and enjoyable means of sharing information, thoughts, opinions and insights on public policy issues likely to impact providers of affordable housing, aging services and post-acute/long-term care. 

{kind=link}
The core challenge is in the one size fits all model of healthcare that currently exists. The system as a…
Reblogged this on rennydiokno.com.
I think you're absolutely right, Scot. We've passed the point of no return on Federal dysfunction.
It sounds like violence can change one's mind about what is right and what is wrong. I always thought that…
The important issue is not the comment that Gruber made rather the fact that he and the administration intended to…